Shall I re-arrange your face?
Pop Quiz – do the bones of the skull in an adult move on a regular basis, or are they fused? What do you think?
Grab a nearby adult and put your fingers in their ears, pushing up and back against the boney bit, and notice if the bones are level, and if not, which side is low (make sure the head is straight first!) Or put your fingers just under the cheekbones on either side of the nose and notice if they are level.
Then lie your adult down on their back, and measure again. Do you get the same results? Did anything switch around, so the side that was high while standing is low while lying down? It won't take many people before you notice that the bones are shifting. Doing that experiment proved to me that the bones of our cranium are not the least bit fused.
I found it astonishing how much the bones in the skull can move, just from standing to lying down, let alone what may happen when one hits one's head in a car crash or when one's face becomes a punching bag.
If you have seen MRI brain scans, you may have noticed that even if the report notes that nothing is wrong – no brain tumour etc. – that the brain may not look symmetrical. This scan is actually pretty good. I had previously linked to one that was very assymmetrical, but that link no longer works.
I think these asymmetries should be considered and noted, because the dura mater, the tough outer coating of the spinal cord ascends into the skull and becomes the tentorium cerebelli membrane, and then merges with falx cerebri membrane which separates both halves of the brain.
Both membranes attach the brain to the various cranial bones. So if the cranial bones are not in their optimal alignment, the result will be a distortion in the brain due to a pulling of the membranes.
Does it not make sense that a distortion in the shape of the brain may at the least bring on headaches, and may possibly affect its function?
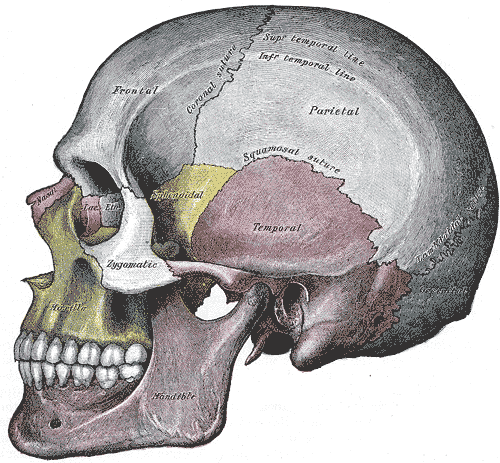
It is not just the outer bones of the cranium that can have an impact. There are many bones that make up our sinuses, which can be easily compromised by bones of the nose and face being out of position. The position of the bone that our upper teeth sit in (maxilla), the lower jaw bone (mandible), and the temporal bone can all have a huge impact on the ability of the jaw to function correctly (TMJ problems).
{kind=link}
{kind=link}
{kind=link}
Because of this, orthodontists need to be very careful when tightening braces not to tighten them to the point that the temporal bones move, as the bite will be altered. (As parents you can check the temporal bones by using the fingers in the ears technique described above. Check before the appointment, and before you leave the orthodontist's office so the braces can be loosened if necessary.)
Seven different bones form the socket of the eye. Many bones have grooves or holes through which nerves and blood vessels feed, and tilts or rotations in the bones may put mechanical stress on those structures.
Of all the bones in the skull, a good position of the sphenoid bone is probably the most important as almost all other cranial bones join with it, impacting the position of the other bones as well. It is a butterfly-shaped bone that goes through the skull at the level of the temples.
{kind=link}
The pituitary gland sits in the center of the sphenoid bone, and produces growth hormone, thyroid stimulating hormone, luteinizing hormone, follicle stimulating hormone, and oxytocin to name just a few, and the pituitary gland sends messages to other endocrine glands to produce hormones too.
So it is possible that poor bone position can affect hormone production as well.
The good news is that if the bones of the head are stuck in a crooked position creating compression through the brain, possible migraine headaches and even brain function problems, it is possible to release the bones without surgery, decompress the areas that compressed, and straighten out the cranium.
Once again, our structure needs to be optimized in order to optimize our function and reduce pain. So if you are in the Vancouver area, come see me and I'll re-arrange your face! 😉
If you want to search for other posts by title or by topic, go to www.wellnesstips.ca.
Related tips
"It's all in your head – I mean neck!"
Posture, leg-length discrepancies, musculoskeletal pain and organ function
Walking, sacroiliac joint dysfunction and hip pain
Pain and stabilizer vs. mover muscles
Shoulder-blade position and neck, arm and upper back pain
St. John, Paul "Welcome to Integrative Balancing of the Atlas-Axis" in Neuro 1 Manual Neurosomatic Educatoris Inc, 2008.
Clark, Randall & Jones, Tracy Neuro ALP 1 Manual Neurosomatic Educators Inc. 2007.
Oleski SL, Smith GH, Crow WT.
Radiographic evidence of cranial bone
mobility. J Craniomandib Pract. 2002;20(1):34-38.
Rothbart, Brian Vertical Facial Dimensions Linked to Abnormal Foot Motion Journal of the American Podiatric Medical Association Volume 98 Number 3 189-196 2008.
Gautam P et al. Stress and displacement patterns in the craniofacial skeleton with rapid maxillary expansion: a finite element method study. Am J Orthod Dentofacial Orthop. 2007 Jul;132(1):5.e1-11.
Jafari A et al. Study of stress distribution and displacement of various craniofacial structures following application of transverse orthopedic forces–a three-dimensional FEM study. Angle Orthod. 2003 Feb;73(1):12-20.
Heisey SR, Adams T.Role of cranial bone mobility in cranial compliance.
Neurosurgery. 1993;33(5):869-876.
Smith, Gerald H. CRANIODONTICS
New technology of the twenty-first Century International Center for Nutritional Research
Blum CL Biodynamics of the cranium: a survey. Cranio. 1985 Mar-May;3(2):164-71.
Online at The Cranial Academy
Copyright 2008 Vreni Gurd
To subscribe go to www.wellnesstips.ca
{kind=link}